QUESTION 1: The stellate ganglion:
A. is a fusion of the inferior cervical and first thoracic ganglia
B. receives fibers whose cell bodies are located primarily at the C4-C7 levels of the spinal cord
C. is primarily a parasympathetic ganglion
D. lies at the level of the fifth cervical vertebra
E.. may be blocked with little danger of complications
QUESTION 2: The most superior approach to the brachial plexus involves placing the needle:
A. between the lateral head of the sternocleidomastoid muscle and the anterior scalene muscle
B. between the medial and lateral heads of the sternocleidomastoid muscle
C. between the anterior and posterior scalene muscle
D. between the anterior and middle scalene muscle
E. on the first rib
QUESTION 3: The obturator nerve:
A. is unimportant in arthroscopic surgery of the knee
B. supplies motor innervation to the adductor muscles of the hip
C. supplies sensory innervation to the skin overlying the patella
D. is derived from the first and second sacral roots
E. supplies sensory innervation to the lateral aspect of the knee
(answers at bottom of post)
___________________________________________________________________________________________________________________________________
REGIONAL ANESTHESIA: BLOCKS
*This is a summary/overview of Regional Blocks based on Nagelhout Nurse Anesthesia. Please click on the NYSORA link (
www.nysora.com) to read step-by-step procedures. Future posts will focus more indepth on individual blocks*
*Click on photos to start familiarizing yourself with nerve anatomy*
-Permits the patient to retain upper airway and pharyngeal reflexes while providing surgical anesthesia.
-Block of SANS results in increased gastric and intestinal motility causing the stomach to empty sooner
-Hypotension that develops from regional may cause increased nausea and vomiting
-Should not be considered an alternative to securing the airway. If airway cannot be secured in a safe manner regional should be avoided
ABSOLUTE CONTRAINDICATIONS:
patient refusal*
uncorrected coagulation deficiencies
infection at site of block
severe bleeding with or without hypovolemia or potential for severe bleeding
trauma and other conditions that cause contracted volume states can result in significant hypotension and tachycardia after initiation of regional
hypovolemic shock
abruptio placentae with or without fetal distress
RELATIVE CONTRAINDICATIONS:
patient age – recommended in neonates; peds provides postop pain management à but should be avoided in children who are unable to tolerate loss of feeling and strength in legs (age 3-9; anxiety)
pts who have difficulty understanding the procedure or who are uncooperative
history of headaches or backaches
pts with chronic neurologic disorders
history of documented LA allergy (a true allergy is rare) – reaction may be d/t a preservative or PABA (para-aminobenzoic acid) a metabolic product of LA hydrolysis. Or may be from LA that contains epinephrine. If they are allergic to an ester, choose and amide. Premedicate with H1 & H2 blocker.
history of Mobitz type I, Mobitz type II or 3rd degree heart block without a pacemaker
patients with fixed-volume cardiac states (unable to respond to changes in SVR by increasing SV as a means of maintaining CO
COMPLICATIONS:
CV problems are the most critical immediate complications
respiratory and GI consequences
immediate and delayed complications
Immediate: potential of intravascular injection à CNS toxicity (tingling of lips, strange taste in mouth, ringing in ears, visual disturbances, seizures); cardiac dysrhythmia (ventricular); respiratory and CV collapse
Complications with Continuous peripheral nerve blocks: nerve injury, bleeding requiring surgical intervention, catheter-associated infection, dyspnea, pneumothorax, LA toxicity, local inflammation at catheter insertion site, equipment failure (broken needles, broken/sheared catheters, glass in the epidural and SA space, injection of wrong drugs)
Techniques used for Regional Blocks:
- Peripheral nerve stimulators
- Ultrasound-guided
UPPER-EXTREMITY BLOCKS:
4 Primary approaches to block the brachial plexus:
1. Axillary
2. Interscalene
3. Supraclavicular
4. Infraclavicular
*Axillary is most frequently used
BRACHIAL PLEXUS ANATOMY:
Brachial plexus is a large network of nerves that extend from the neck through the xilla and innervate the upper extremity
(click image to enlarge)
Composed of ventral rami (roots), trunks, divisions, cords and their branches.
(Randy Travis drinks cold beers)
(click image to enlarge)
Supraclavicular portion: 5 ventral rami, 3 trunks, 6 divisions
(lies in posterior triangle of neck)
Infraclavicular portion: 3 cords, 4 branches (lies in axilla)
(click image to enlarge)
BP passes between anterior and middle scalene muscles, through posterior triangle of the neck and into the axilla, where they end in the 4 branches that supply upper extremity
RAMI/ROOTS
- -Originate from C5-T1; small % of individuals arise from C4 or T2
TRUNKS
- The 3 nerve trunks (superior, middle, inferior) are enveloped by a fascial “sheath” – arises from fascia of anterior and middle scalene muscles à forms the interscalene space
DIVISIONS
- 6 divisions can be divided further into 3 ventral divisions and 3 dorsal divisions
- Ventral divisions: supply ventral (flexor) portion of upper extremity
- Dorsal divisions: supply dorsal (extensor) portions of upper extremity
CORDS
- 3 cords: posterior, lateral, medial – named according to their position in relation to the axillary artery
- Lateral à divides into muscularcutaneous nerve and portion of median nerve
- Medial à ulnar nerve and portion of median nerve
- Posterior à axillary nerve and radial nerve
NERVE BRANCHES
Branches of lateral and medial cords (median, ulnar, musculocutaneous) predominately supply ventral portion of upper extremity
Posterior cord (radial, axillary) supply dorsal portion of upper extremity
Posterior portion of fingers and hand, considerable cutaneous representation of the “predominantly ventral” median and ulnar nerves
- Radial nerve (C5-C8, T1) is major nerve supply to dorsal extensor muscles (triceps) of upper limb below shoulder, sensory innervation to extensor region of arm, forearm, and hand.
- Musculocutaneous (C5-C7) supplies flexor muscles (biceps, brachialis, coracobrachialis) of ventral portion of arm; supplies sensory to lateral aspect of forearm btwn wrist and elbow as the lateral antebrachial cutaneous nerve.
- Median and ulnar nerves pass through arm and provide sensory and motor innervation to forearm and hand
- Median (C6-T1) supplies flexor and pronator muscles; sensory to ventral portion of thumb, first and second fingers, lateral ½ of third finger, palm of hand
- Ulnar (C8 and T1) supplies motor to most of small flexor muscles. No sensory innervation of forearm; sensory to medial part of third finger, entire 4th finger and remaining portion of palm of hand
APPROACHES TO BRACHIAL PLEXUS BLOCK:
Choice of approach should be based on patient considerations, location of planned surgical intervention and skill and experience of the practitioner.
For surgery at or below elbow (hand, forearm)
Limited rang of motion of extremity (fracture – pain) can limit access to axilla and use of this block
(click image to enlarge)
Clockwise from musculocutaneous --> Median --> Ulnar --> Radial
Mc-M-U-R
(click image to enlarge)
Can use one of 3 techniques:
· Loss of resistence
· Penetration of axillary artery
· Elicitation of paresthesia
Most proximal brachial plexus block; used for surgery involving shoulder and proximal humerus; only technique that can provide anesthesia to shoulder and rest of upper extremity.
(click image to enlarge)
Three trunks of the cervical plexus are revealed lying alongside the subclavian vessels
Catheter is placed at level of trunks
(click image to enlarge)
SUBCLAVIAN APPROACH
Subclavian artery palpated behind midpoint of clavicle (palpate 1-2 cm above clavicle); advance needle here perpendicular to skin
*Must watch for onset of
Horner syndrome (triad of miosis, partial ptosis, and loss of hemifacial sweating) as a positive sign of a successful block.
Complication: pneumothorax (pleura of lung is immediately inferior to first rib)
(click image to enlarge)
The needle enters the sheath of the brachial plexus at the farthest possible distance from the SC artery
(click image to enlarge)
The patient is placed in the supine position with the head supported and turned toward the opposite shoulder.
INTERSTERNOCLEIDOMASTOID APPROACH (ISCM)
Newest supraclavicular approach; puncture site situated between heads of SCM muscle
Decreases incidence of Horner syndrome and pneumothorax associated with subclavian approach
Brachial plexus reached at level of trunks; Needle passes between heads of SCM, behind clavicular head, through middle cervical fascia, next to phrenic nerve, through anterior scalene before arriving at brachial plexus
Puncture site is 2 fingerbreadths above sternal notch, btwn heads of SCM, medial to clavicular head.
SELECTIVE BLOCKS AT THE ELBOW:
Primarily sensory blocks; pt can still move
When a tourniquet is used during surgery, the intercostobrachial nerve and brachial cutaneous nerve should be blocked in the axilla à permit patient to tolerate tourniquet Coracobrachial muscle can also be blocked at level of shoulder to tolerate tourniquet
1. ULNAR NERVE BLOCK AT ELBOW:
Ulnar nerve traverses ulnar sulcus of humerus; < 3 ml to prevent ischemia of nerve
Performed 1-2 cm proximal to sulcus
Identify medial condyle of humerus; insertion point of needle is between medial condyle of humerus and olecranon process of ulna
If paresthesia is elicited on introduction of needle, withdraw needle 1 mm and inject 2-3 ml of LA
(click image to enlarge)
The pts elbow is flexed 90 degrees and the medial condyle of the humerus is identified.
2. MEDIAN NERVE BLOCK AT ELBOW:
Anesthesia of forearm and hand can be done with combination of median and ulnar nerve block
Median nerve block can supplement partially successful brachial plexus block
Should be avoided in pts with carpal tunnel syndrome, neuritis, or perforated artery
Needle inserted slightly medial to brachial artery at depth of 0.5-0.75 cm
(click image to enlarge)
Performance of median nerve block, positioning pts arm on a stable surface with the elbow slightly flexed. After brachial artery is identified, a short needle is inserted slightly medial to the brachial artery.
3. RADIAL NERVE BLOCK AT THE ELBOW
Radial nerve is located in groove formed by fascial border of brachioradialis muscle on lateral edge and biceps tendon medially
Anesthesia for outpatient or supplement to brachial plexus anesthesia; only sensory
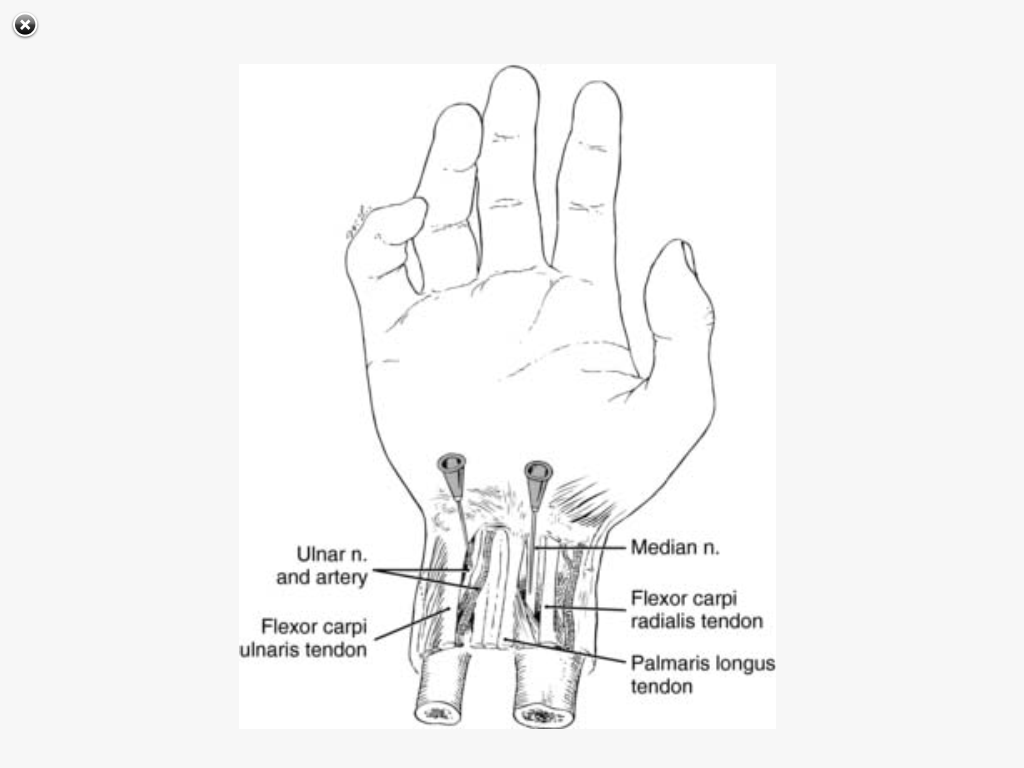
1. ULNAR BLOCK AT THE WRIST
(click image to enlarge)
With the pts wrist slightly flexed and stabilized on a firm surface, the ulnar flexor muscle of the wrist is identified. A short needle is inserted perpendicular to the skin on the radial side of the ulnar flexor muscle of the wrist.
2. MEDIAN BLOCK AT THE WRIST
3. RADIAL BLOCK AT THE WRIST
(click image to enlarge)
Anesthesia of radial fibers is achieved by injecting a subcutaenous ring of LA solution at the radial flexor muscle of the wrist, extending to the dorsal surface of the ulnar styloid.
BIER BLOCK: INTRAVENOUS REGIONAL ANESTHESIA (
Nysora link)
Best for upper extremity (hand, wrist) soft-tissue surgery of < 1 hr; can be used for lower extremities
Requires use of a tourniquet
Potential for rapid transfer of large volume of LA from extremity to central circulation – have emergency equipment available
- Apply tourniquet but keep deflated
- elevate extremity and exsanguinate by wrapping Esmarch bandage from fingers to tourniquet
- inflate tourniquet to 100 mmHg above SBP (or 250 mmHg); remove bandage
- inject 50 ml of 0.5% lidocaine via IV – preservative free, no epi
- can use additional tourniquet (Penrose drain) for faster onset and denser block
- can add 15 – 30 mg of ketorolac to LA soln
Indications for lower extremity IV regional anesthesia include orthopedic surgery of short duration on foot, removal of fixation plates and screws from bones below the knee, foreign body removal from foot.
Anatomic landmarks easily identified; no extremely painful, high success rate, low complications
Most common complications: pneumothorax and toxicity from LA
Pt who has pain with respiratory effort is able to cough and breathe deeply with reduced pain.
High vascularity of area and large intercostal veins contribute to high plasma level of LA
Pt position can be prone, lateral or sitting
Intercostal nerve emerges from intervertebral foramen and follows rib in the costal groove. This groove is located in anteroinferior aspect of rib. The intercostal artery and vein accompany nerve in this groove.
Catheter can be inserted.
Tachyphylaxis can develop; use a different class of LA (ester or amide)
LOWER EXTREMITY BLOCKS
Anatomy of Lumbar Plexus
Formed from L1-L4; contributions from T12. Formed in front of quadratus lumborum muscle and behind psoas major muscle.
The lateral femoral cutaneous nerve is formed from L2-L3 and is first to leave compartment. It emerges from lateral border of psoas major at its midpoint. Then traverses iliac muscle obliquely toward anterior iliac spine. Passes under lateral border of inguinal ligament and provides sensory innervation to the lateral aspect of the thigh.
The obturator nerve arises from L2-L4 as an extension of the lumbar plexus. Emerges from medial border of psoas major at level of sacroiliac joint and is covered by external iliac artery and vein. Passes into pelvis minor and runs anteroinferiorly to obturator canal which it traverses near obturator vessels. *Because of the proximity of the nerve to the external iliac artery, it can be injured during surgical procedures. Frequently injured during pelvic surgery. Obturator nerve is primarily a motor nerve that has some mixed sensory fibers to hip, medial aspect of femur, and skin and soft tissue of lower portion of thigh.
The femoral nerve is formed from L2-L4 is at junction of middle and lower 1/3 of psoas major muscle. Remains within the groove of the psoas major and iliac muscles and runs deep under the inguinal ligament where it comes anterior to iliopasoas muscle and lateral to femoral artery. Forms 2 branches: anterior and posterior bundles.
Anterior branch provides innervation to anterior surface of thigh and sartorius muscle.
Posterior branch provides innervation to quadriceps muscles, knee joint, and its medial ligament and is the origin of the saphenous nerve.
*Femoral nerve is encased in a sheath anatomically similar to brachial plexus - same techniques used in upper extremities can apply here.
PSOAS COMPARTMENT BLOCK (Nysora link)
Blockade of the lumbar plexus as a unit can be accomplished by injecting LA into the fascial sheath surrounding the plexus. This can be done at the level of the psoas compartment.
This approach attempts to block the plexus as it lies in the fascial plane bordered medially by the vertebral column, dorsally by the quadratus lumborum muscle, and ventrally by the psoas major muscle.
INGUINAL PERIVASCULAR TECHNIQUE AND FEMORAL NERVE BLOCK (
Nysora link)
This is also known as the
three-in-one block, or
Winnie's block.
The lumbar plexus is "sandwiched" among the psoas major, quadratus lumborum, and iliacus muscles and is enclosed by the fascia of these three muscles.
Complication:
infection of deeper tissues
(click image to enlarge)
Site of injection is 1 cm lateral to femoral artery and 1 cm inferior to inguinal ligament. Volume 30 ml
CONTINUOUS FEMORAL NERVE BLOCK
Similar to previous block but catheter is inserted 5-10 cm beyond tip of needle. Continuous infusion of LA is initiated after 15-20 ml bolus injection at a rate of 8-10 ml/her.
0.2% ropivacaine or 0.25% bupivicaine
FASCIA ILIACA COMPARTMENT BLOCK
An anterior lumbar plexus approach with a punture point distant from neurovascular sheath. Used widely for postop analgesia after lower limb surgery in children and adults after hip, femoral shaft, or knee surgery.
*Compared to 3-in-1 block, it provides fater and more consistent simultaneous blockade of lateral femoral cutaneous and femoral nerves
SCIATIC NERVE BLOCK
Sciatic nerve, in combination with lumbar plexus, femoral and saphenous nerve blocks, provides complete anesthesia and postop analgesia for lower-extremity surgery.
*Posterior and lateral popliteal approaches most commonly for ankle and foot surgery
*Higher approaches to sciatic nerve are more commonly for surgery below, above and at the knee.
Anatomy: Sciatic nerve is the continuation of the upper division of the sacral plexus and is the largest nerve trunk in the body. Supplies the muscles of the back of thigh, skin of the leg, and muscles of lower leg and foot. Passes out of the pelvis through the great sacrosciatic foramen below the piriform muscle. Descends between the major trochanter and tuberosity of the ischium to the lower 1/3 of the thigh, where it divides into the internal and external popliteal nerves.
(click image to enlarge)
A line is drawn from posterior superior iliac spine to greater trochanter of femur. 2nd line is drawn from sacral hiatus to greater trochanter, and 3rd line is drawn perpendicular to and bisecting the first line. Intersection of 2nd and 3rd line is point of needle entry.
POPLITEAL FOSSA BLOCK (Nysora link)
Use of 3 anatomic landmarks that define the posterior popliteal fossa: popliteal crease, medial border of femoris biceps muscle laterally, and tendon of semitendinous muscle medially.
(click image to enlarge)
Popliteal nerve block
A line is drawn joining the medial border of the femoris biceps muscle laterally and the lateral border of the semiteninous muscle medially at the level of the popliteal crease. From the middle of this line, a perpendicular line is extended 15 cm cephalad. This site of insertion of the needle is 1 cm laterally.
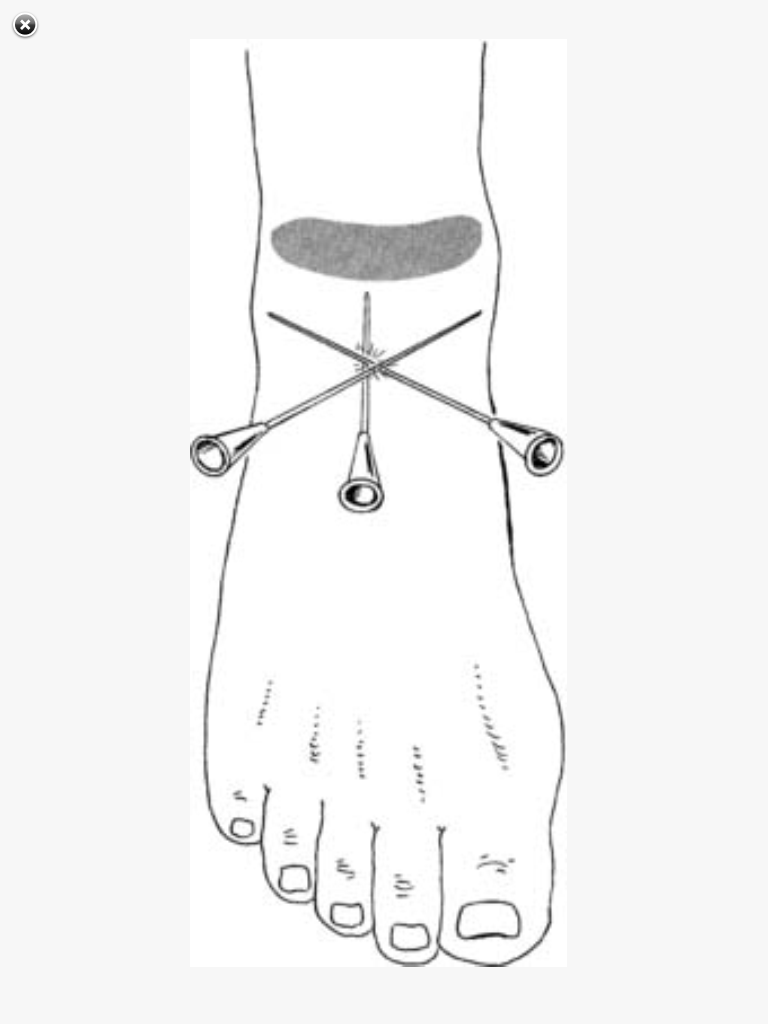
ANKLE BLOCKS (Nysora link)
For patients requiring surgery of the
foot, not ankle. (i.e. gangrene or diabetic foot ulcer)
Done by blocking 5 nerves at level of the ankle: tibial, sural, superficial peroneal, deep peroneal, saphenous.
(click image to enlarge)
Direction and redirection of needle in ankle block technique
Tibial Nerve
Arises from nerve roots of L4-L5 & S1-S3
Path lies on medial side of Achilles tendon. Passes into ankle with the posterior tibial artery. Nerve lies behind artery and between the tendons of the long flexor muscles of the toes and the long flexor muscles of the great toe. Several branches leave the neural bundle at the level of the medial malleolus. Has 2 braches: medial and lateral plantar nerves. Provides sensory innervation to foot.
(click image to enlarge)
Path of the posterior tibial nerve, with the posterior tibial artery past the Achilles tendon
Sural Nerve
Formed from the union of a branch of the tibial nerve and the common peroneal nerve. Travels superficially with the short saphenous nerve behind the lateral malleolus into the ankle, where it provides sensory innervation to the posterior portion of the sole of the foot, and posterior portion of heel, and portion of Achilles tendon immediately above the ankle.
(click image to enlarge)
Path of the sural nerve behind the lateral malleolus in the ankle
Superficial Peroneal Nerve
Arises from L4-L5 & S1-S2
Nerve becomes superficial in middle 2/3 of the lower leg and remains subcutaneous as multiple braches proceed into the dorsum of the foot. Just above the ankle the nerve begins to branch - for this reason, a single injection site does not provide sufficient anesthesia
(click image to enlarge)
The superficial peroneal nerve proceeds to the dorsum of the foot subcutaenously through multiple branches
Deep Peroneal Nerve
Arises from same nerve roots at superficial peroneal nerve.
Remain inside anterior tibial muscle and long extensor muscle of great toe as it traverses leg into ankle. Provides innervation to short extensors of toes and sensory to skin on lateral side of hallux and on medial side of second digit. Nerve and artery cross each other so the nerve lies lateral to the anterior tibial artery and medial to long extensor muscle of the great toe that is in the ankle.
*This nerve if frequently missed when regional is administered to the ankle.
Saphenous Nerve
This is the terminal branch of the femoral nerve and travels subcutaneously from lateral side of knee joint. Follows the greater saphenous vein to the medial malleolus and provides
sensory innervation to medial side of malleolus and skin of the medial aspect of the lower leg
*If the block of this nerve is inadequate, pt is unable to tolerate a tourniquet above the ankle.
ANSWER 1: (A) The stellate ganglion is a fusion of the inferior cervical and firsth thoracic ganglia and lies at the level of the 7th cervical vertebra. The ganglion is a sympathetic ganglion and receives fibers whose cell bodies are located at T1-T8 levels of the spinal cord. Stellate ganglion block has many potential complications, including pneumothorax, intravascular injection, and subarachnoid injection
ANSWER 2: (D) The most superior approach to the brachial plexus is the interscalene block in which the needle is inserted between the anterior and middle scalene muscles
ANSWER 3: (B) The obturator nerve supplies motor innervation to the adductor muscles of the hip and sensory innervation to the medial aspect of the knee
REFERENCES:
McGraw-Hill Specialty Board Review
Nagelhout, Plaus. Nurse Anesthesia
NYSORA.com